
It was a day after I had been granted access to the treatment facility for Covid-19 positive persons at the University of Ghana Medical Centre (UGMC).
We were unsuccessful at seeing the Intensive Care Unit (ICU) of the facility which at the time was treating three critically ill COVID positive persons.
Head of the ICU and National coordinating member for severe and critical cases, Dr. Chris Owoo had asked our team to return only after I had personally fulfilled my part of a deal we struck.
[I'm not letting out details of this one, I would not give. Tongue-in-cheek]
But long story short, Friday, April 24, we would have another exclusive tour - this time of the ICU.
What comes to mind readily when you hear ICU?
I was to discover it all that day and of course in the context of Covid-19.
It's an elevated floor of the patient tower at the UGMC (I think the second floor, or so).
I cannot immediately remember because finding the entrance of the unit got us going round in circles for quite a bit.
We didn't need to be told we had found the ICU after five minutes. The glassware had boldly inscribed on it …"ISOLATION AREA. INTENSIVE CARE UNIT."
The foyer before the ICU smelt typically like a hospital - drugs, disinfectants.
"…Welcome here. We will try as much as possible to give you a bird's eyeview of the unit, inasmuch as we would be professional not to expose the identities of our vulnerable patients", Dr. Owoo mentioned.

He came to meet us flanked by a host of critical care staff - Dr Sottie in particular appearing and sounding quite unsettled by our presence.
I know how these things go sometimes, especially for persons who are not used to the cameras.
Donning!
With my experience at the donning area the day before with Dr Amoah and Dr Edwin, I knew I was a pro.
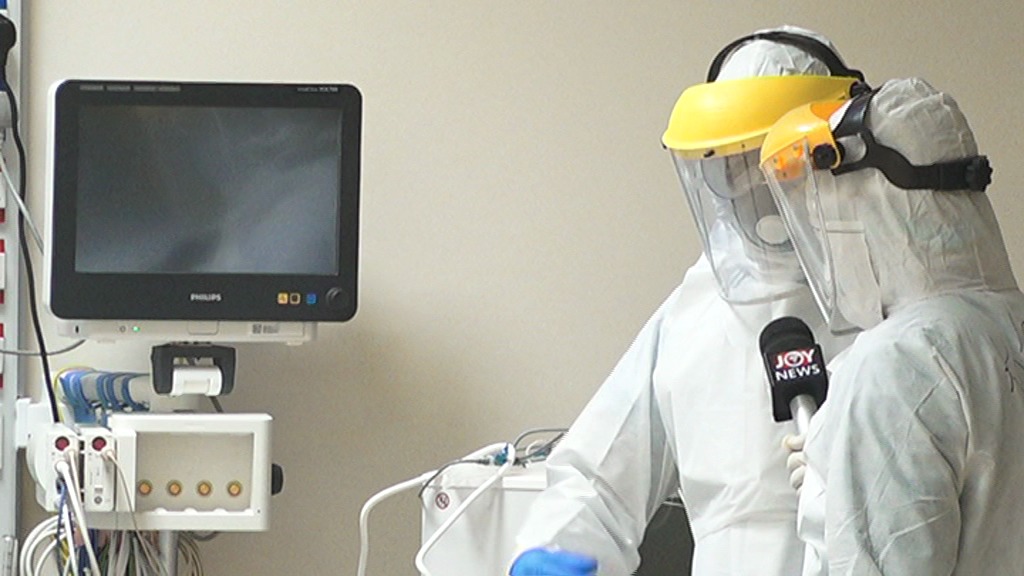
But it looked even more cumbersome here. Dr Emma Anima Addae and Dr Daniel Sottie are preparing to get inside the ICU to offer critical care to the three persons in there who were being assisted to survive.
They rub their hands with alcohol - they wear their coveralls, their boots, masks, aprons, goggles and an extra layer of facial protection - the face shield.
If I would be accurate in my timekeeping, I bet it took them more than twenty minutes - but I did 35 minutes.
Dr Owoo like a narrator, explained each stage and the need for each material used at the donning area.
Lordina, one of the senior nurses was already fully donned when we got here.
It was time to go in and feed the patients, administer some medication and check their vitals.
Three container wraps of food are handed to her, accompanied by quite a number of instructions read out from a tiny little piece of paper by the Deputy Director of Nursing Services (DDNS).
She would have to do these and more depending on further instructions from the monitoring room of the ICU.
Inside the ICU proper
The picture on my mind - dramatic scenes. Patients barely surviving. Care staff running around in circles. Monitoring devices beeping (beep-beep) every 2 seconds.
But Inside here was different.
More than twenty beds are here. Lordina already inside on care duties. Dr Anima Addae and Dr Daniel Sottie are on opposite ends of the room.
Farther up, is a bed with a man being fed, close to an empty bed where Dr. Sottie and I stood having a conversation about ventilators and oxygen masks and suction devices etc.
I'm sure he would have realised briefly that I was stealing consistent glances in the areas where these three patients were.
My cameraman was behind the door. Unlike the regular treatment area, a camera would not get inside the ICU; an area tagged the red zone or the contaminated area.
And so in the extreme ends of the room where the patients lay, Seth Tenge's lenses would not be able to make the slightest capture.
Occasionally, they will come to a zone and remove their gloves and wear another pair.

P.S: Each care staff wears two layers of hand gloves before getting inside and then they wear another pair as another layer of protection.
Dr Addae says, "this is imperative to avoid contamination and transferring the viral load from one patient to another even though they are all Covid-19 positive."
With their kind of work, they touch the patients, they turn them around, they administer drugs, they help them onto life support devices and all, they are exposed if they do not adequately protect themselves with the gear.
Mr M from where I stand is helped to sit up on the bed - he looked in some discomfort. He winces and adjusts his body up across an elevated table to feed.
It almost took my attention away from what Dr. Sottie was telling me - I guess he was explaining how patients are put on ventilators and what role these devices play in offering life support to critically Ill patients.
The telecom device in the ICU rings.
Dr Addae moves to pick up - their boss Dr. Owoo wants them to conduct an ECG (nothing to do with electricity distribution in our homes).
An electrocardiogram (ECG) is a medical test that detects cardiac (heart) abnormalities by measuring the electrical activity generated by the heart as it contracts.
That is what Dr Sottie and Addae are to conduct - the third one. Two previous ones taken have their results ready.
"..Dr Joseph Akaamah the intervention cardiologist with Korle-Bu Teaching Hospital is on his way here to review the results. Do that quickly and in about a minute or two he would be here, OK?.
Dr. Owoo said via the communication device.
"..He is climbing up, once he gets here you would display the results of the three ECGs so we take it up from there," he said.
I had been told minutes prior that Mr R had had a cardiac condition overnight - a reason the cardiologist was called in.
Before long Dr Akaamah was at the door. The electrocardiograph had recorded Mr R's third ECG and Dr Addae and Dr Sottie had copies to give to the cardiologist.
But how was it going to be done. Certainly these papers with the ECG results would not go out of this room, I had been told.
"…nothing leaves this room once they get here, remember? Dr Addae reminded me.
"…We will display the three results on the glass door. The cardiologist would take a photograph with his phone from behind the door. And then later review the results."
It looked to me like a strange exercise - but it is normal here.
Before long, the behind-the-door review was concluded and it was time to leave the chilling cold ICU room.
But despite the temperature here, I was gasping for breath. I was almost suffocating beneath the nose mask.
My goggles were foggy. My forced breathe had clouded the surfaces.
It had been more than an hour inside this place. But that's in no way compared to the several hours some of these critical care staff spend inside the ICU.
Lordina is still inside. She was moving onto another patient when we left with Dr Sottie and Addae.
Doffing process
As the automated glass door slid shut behind us, another official standing before us held in hand what looked like a knapsack spayer and a stick.
This was a process of literally giving us a chlorine bath.
She pumps the chlorine inside the sprayer and with a trigger she sprays the content carefully on our coverall…touching every part.
Beneath our boots, our hands with two layers of gloves, our face with the goggles and everything.

My microphone and the boom stick also was chlorinated.
The concentration of this chlorine solution is 0.5.
It is a perfect decontamination agent.
And one after another under the watchful eyes of a supervisor, we removed our PPEs and cleaned up with yet another chlorine solution - this time with concentration at 0.05.
This is a stage where the possibility of contamination rises by several notches. Therefore it is carefully and professionally supervised.
"..However exhausted you may be from wearing the PPEs and working inside the ICU, you need a great deal of patience to doff off," Dr Addae told me.
Sign off
It's been another day. In fact, five hours filming this. I was already laboured. But this is the life of critical care staff here at the UGMC ICU.
It's been their life since COVID.
Dr. Chris Owoo says, "its even tougher now because we have to stay away from home, sometimes we get home after midnight. Our families are having a challenge dealing with it".
The psychological hump is also telling. But "we reassure them that this too shall pass.".
Dr Anima Addae has had to separate herself from her family. She tells me she has parents who belong to a high-risk group.
"…if they get the infection they belong to the high risk group and so I have had to separate from them and live alone."
"When we close, we cannot use public transport anymore because you do not want to risk the larger population because of where you work in the treatment center."
All aspects of their lives have changed.
"We do not follow the figures like most of you do. We cannot do social media because we are working. Our shifts are long."
They have had to make several adjustments to their lives, their social interactions, their every day work ethic.
Some of their colleagues declined to work in the treatment centres because of the risks.
But Dr Sottie after his initial fear of working here has settled in. He did not think he could do this especially at a time Europe was being heavily battered by the virus.
Today, he calls for the support of the public to help in this battle.
"…while we do our part as health workers, we want the citizens to also do their part. And to pray for us. It is not by our might that we do what we do."
"I look forward to a time we would all come together as a nation and celebrate after this is all gone, but for now, the public should do their part and stay home."
These were words from deep within them; I could see passion while they spoke them.
It was in their eyes. For those who still at this stage believe COVID-19 is a hoax, these critical care staff say "IT IS REAL".
They do not gloat in making these drastic changes to their own lives over nothing. It is a course they have signed up for and are willing to give off their best and stand in the gap for us.
Let us help them by doing our part.
I pledge to stay distant, stop the spread and also to abide by the safety protocols that have been recommended to us.
It is my own small way of helping these MVPs Dr. Owoo, Dr. Addae, Dr. Sottie, Dr Edwin, Dr Amoah, Lordina, and all the others like them, to fight this battle for us.
This is their story!
Latest Stories
-
Trinity Oil MD Gabriel Kumi elected Board Chairman of Chamber of Oil Marketing Companies
25 minutes -
ORAL campaign key to NDC’s election victory – North America Dema Naa
43 minutes -
US Supreme Court to hear TikTok challenge to potential ban
48 minutes -
Amazon faces US strike threat ahead of Christmas
1 hour -
Jaguar Land Rover electric car whistleblower sacked
1 hour -
US makes third interest rate cut despite inflation risk
2 hours -
Fish processors call for intervention against illegal trawling activities
2 hours -
Ghana will take time to recover – Akorfa Edjeani
2 hours -
Boakye Agyarko urges reforms to revitalise NPP after election defeat
3 hours -
Finance Minister skips mini-budget presentation for third time
3 hours -
‘ORAL’ team to work gratis – Ablakwa
3 hours -
Affirmative Action Coalition condemns lack of gender quotas in Transition, anti-corruption teams
3 hours -
December 7 election was a battle for the ‘soul of Ghana’ against NPP – Fifi Kwetey
3 hours -
Social media buzzing ahead of Black Sherif’s ‘Zaama Disco’ on December 21
3 hours -
Afenyo-Markin still suffering from the massive defeat – Fifi Kwetey
3 hours